Swimming, tennis, volleyball, javelin throwing, baseball and handball have one thing in common: they are among the so-called “overhead sports” that increase the risk of developing a shoulder – also known as a thrower’s shoulder. also known as thrower’s shoulder. How does this happen, what exactly is thrower’s shoulder? And what can you do if you notice early warning signs?
The thrower's shoulder - a complex clinical picture
The term “thrower’s shoulder” or “athlete’s shoulder” refers to various disease processes and injuries. They mainly affect the complicated joint connection between the humeral head, the glenoid cavity (part of the shoulder blade) and the collarbone as well as the surrounding soft tissue – muscles, ligaments, tendons and joint capsule.
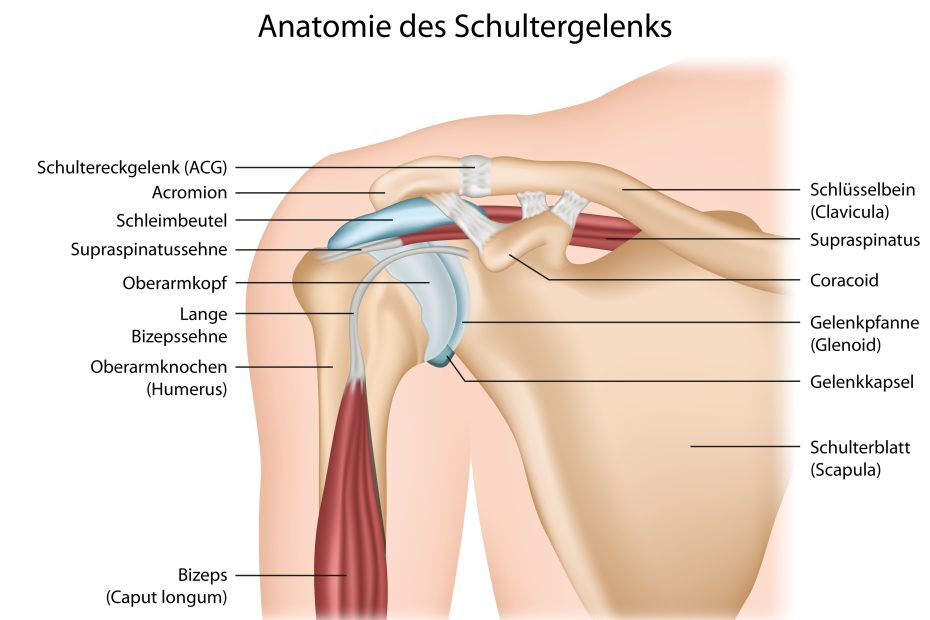
Nerves can also be affected. The clinical picture can include tendonitis and degenerative changes in tendons, partial tears or complete ruptures, muscle shortening, changes to the joint capsule and the resulting movement restrictions, entrapment of shoulder tendons or impaired mobility of the shoulder blade(scapular dyskinesia). Often affected are the biceps tendon, the rotator cuff (a group of four muscles that surround and stabilize the shoulder joint), in particular the tendon of the supraspinatus muscle, which originates from the shoulder blade and runs through the acromion, and the cartilaginous joint lip (labrum) on the lower edge of the socket.
As the shoulder is a ball and socket joint and therefore allows a large range of movement, minor complaints are quickly perceived as very unpleasant under constant strain.
How does a thrower's shoulder / athlete's shoulder develop?
Overhead movements performed repeatedly with force – such as throwing or playing tennis – play a role in the development of an athlete’s shoulder. The first signs of adaptation to this movement pattern can occur at an early stage without causing symptoms, for example changes to the joint capsule.


The one-sided strain leads to stretching of the joint capsule in the direction of external rotation (lunging movement) and shrinkage on the opposite side, resulting in aglenohumeral internal rotation deficit (GIRD). In the development of an athlete’s shoulder, overhead movements performed repeatedly with the use of force – such as throwing or playing tennis – play a role. The first signs of adaptation to this movement pattern can occur at an early stage without causing symptoms, for example changes to the joint capsule: The one-sided load leads to a stretching of the joint capsule in the direction of external rotation (lunging movement) as well as shrinkage on the opposite side, resulting in aglenohumeral internal rotation deficit (GIRD). The shortened capsule on the back causes the humeral head to shift backwards and upwards in the socket. This in itself measurably disturbs normal joint play and can lead to tendon impingement.
Overloading and monotonous movement sequences can also cause small, unnoticed injuries in the muscle and connective tissue, so-called microtraumas. These cause reactive inflammation, which causes pain and swelling and can further damage the tissue over time. The supraspinatus tendon in particular, which passes through a narrow bony-connective tissue tube (acromion) on its way to the humerus, is sensitive to swelling, as it then causes friction with the surrounding structures, which exacerbates irritation and inflammation. Inflammation and tiny hemorrhages caused by micro tears can also lead to the formation of calcium deposits in the muscles or tendon, which also cause pain and restricted movement.
How often does an athlete's shoulder occur?
The studies currently available vary greatly and give a relatively unclear picture of the frequency of occurrence of an athlete’s shoulder in different sports. With a disease risk of 40 to 90 percent, swimmers in particular are at risk of developing corresponding changes and symptoms. Baseball players (60 to 70 percent), tennis and volleyball players (20 to 60 percent) also belong to the risk groups.
Symptoms, progression and prognosis of a thrower's shoulder
Typical symptoms are load-dependent pain and restricted movement during throwing or swimming movements. Internal rotation is restricted compared to the side – it becomes difficult to get the hand behind the back without pain. Affected tendons and tendon insertions are swollen and sensitive to pressure. The pain can be temporarily relieved by resting the hand, but recurs immediately on renewed exertion and worsens if no treatment is given. Over time, the movement restrictions become more pronounced and there is a considerable loss of strength and function. Occasionally, a misalignment of the shoulder blade is visible at first glance when comparing the sides.
If the athlete’s shoulder is not treated, particularly affected tendons such as the subscapularis or supraspinatus tendon can fray and tear partially or completely. In severe cases, the changes can lead to an inability to play sport without treatment. Depending on the complications that occur (e.g. the formation of calcific foci), this can also lead to considerable restrictions in everyday life and at work or to an inability to work. If the pathological changes are detected and treated at an early stage, it is usually possible to regain full fitness for sport. As a general rule, the more pronounced the structural damage to the joint and the surrounding soft tissue, the more complex, complicated and protracted the treatment. The earlier the therapy starts, the better.
Conservative therapy through physiotherapy
Physiotherapeutic treatment also depends on individual functional restrictions and damage. In the early phase, pain relief and treatment of the affected (inflamed) tendons can be the main focus, for example using ultrasound, electrotherapy or transverse friction. Mobilization of the shoulder blade, muscle stretches and stretching of the shortened joint capsule can help to increase the range of movement again and prepare for normalization of the interaction between the shoulder blade, cervical spine and upper arm. The patient also learns stretching techniques that he or she can use independently at home (keyword: “sleepers stretch”). Muscular imbalances – shortened muscles on one side of the joint, weakened muscles on the other – are treated with stretching exercises and active muscle-building exercises. If necessary, a normal position of the shoulder blade must be trained. The joint-stabilizing rotator cuff is also trained before general rehabilitation training can follow to restore the ability to play sports if no complications occur. The trunk and leg muscles are also intensively involved in order to create the best possible static and dynamic conditions for a powerful throwing or swimming movement.
Surgery is required for ruptures and partial ruptures of tendons, damage to the joint labrum or often for symptoms that are resistant to treatment. In such cases, frayed or dead tissue can be removed by means of debridement, for example. Even a partially detached labrum can also be surgically reattached to the bony edge of the joint socket or (partially) torn tendons can be reconstructed. In the vast majority of cases, this is done as part of an arthroscopic procedure (“keyhole surgery“), so that rapid healing is possible.
How can you prevent a thrower's shoulder?
Even if there are no symptoms, “overhead athletes” should have the condition of their shoulder checked by a doctor or physiotherapist. Although a slight restriction of internal rotation does not yet cause any symptoms, it can be an indication of a displacement of the humeral head from the center of the joint – and thus altered sliding movements in the joint. The aim of prevention must be to avoid the combination of capsular shrinkage and muscle shortening that leads to the athlete’s shoulder or thrower’s shoulder. To this end, a self-exercise program can be developed that prevents the development of muscular imbalances and promotes optimal centring of the joint head by the rotator cuff. Even if there are no symptoms, the shoulder should be examined twice a year for pathological changes or consequences of overuse.