The rotator cuff
Rotator cuff tear
Acute care & follow-up treatment
What exactly the rotator cuff is, what functions it has, how to treat an injured rotator cuff effectively and further information on this topic can be found on this page.
ÜBERSICHT
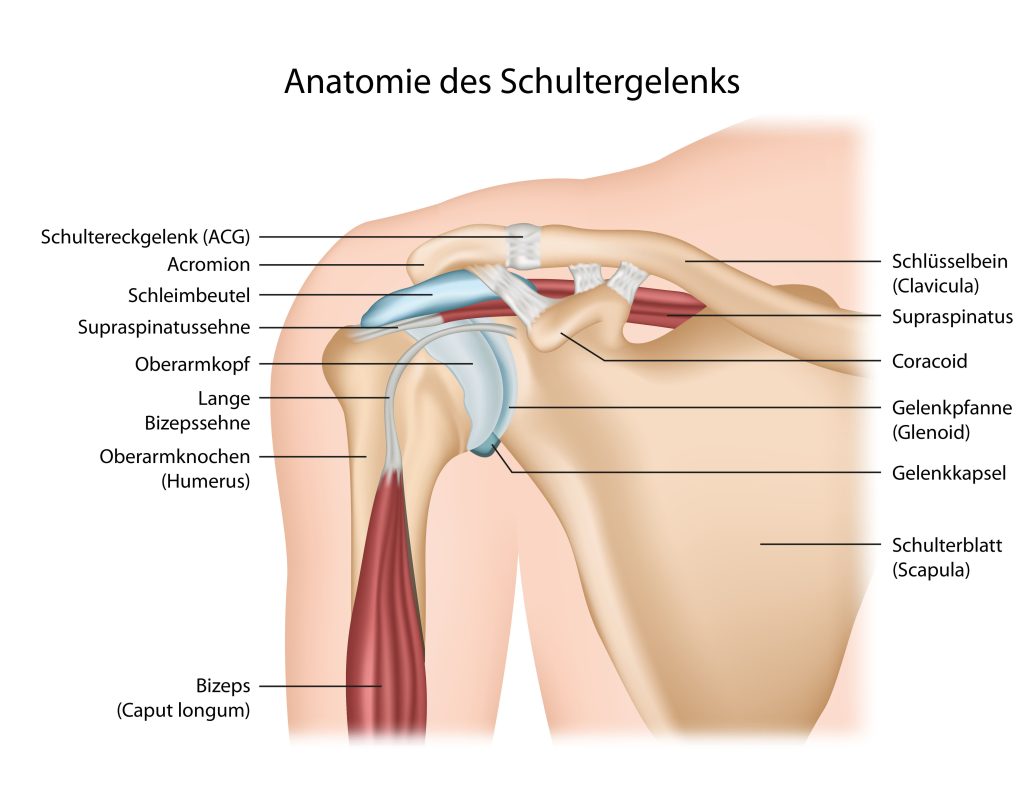
What is the rotator cuff?
The rotator cuff of the shoulder consists of a group of four muscles, all of which originate from the shoulder blade: the subscapularis, supraspinatus, infraspinatus and teres minor muscles. The muscle group surrounds the humeral head or shoulder joint like a cuff and centers it in the shoulder joint. Shoulder socket (glenoid).
In addition to the stabilizing effect of the shoulder joint, these four muscles are mainly responsible for the well-functioning rotation of the humeral head in the shoulder socket – they are therefore responsible for ensuring that the upper arm moves in relation to the shoulder blade. According to their function, they are referred to as ” Rotator cuff” is the term used. A tear of the rotator cuff ( Rotator cuff lesion) can occur as a result of an acute injury (e.g. shoulder dislocation). Much more frequently, however, chronic wear and tear or irritation (e.g. impingement syndrome) leads to degeneration or tear formation. This often progresses gradually and imperceptibly until symptoms suddenly appear, often as a result of minor trauma. Prolonged pain, calcification or irritation often precede the formation of tears.
How do I recognize a rotator cuff tear?
Rotator cuff injuries are typically characterized by pain when lifting the arm, rotational movements and loss of function (pseudoparalysis) of the shoulder if individual parts of the rotator cuff are completely torn. In the case of the supraspinatus, which is usually affected, the affected arm falls limply downwards during the examination after passive lifting and cannot be held in an elevated position against gravity.
Causes and risk factors of a rotator cuff tear
There are two types of rotator cuff tears: those caused by wear and tear(degenerative) and those caused by accidents(traumatic). Traumatic tears are much rarer and usually occur as a result of an accident, for example if you fall on your arm when it is bent or splayed.
The most common cause of this type of rupture in the shoulder is probably acute-chronic damage. This occurs when a small force or jerky movement causes the already damaged tendon(s) to tear away from the bone.
Like all structures in the body, the rotator cuff is also subject to a certain ageing process and the tendon plate decreases in thickness over the years. This can subsequently lead to a rupture. Various factors can accelerate this process, such as increased strain, repeated injuries or smoking. So-called calcific shoulder and subacromial impingement (a phenomenon where the tendon is trapped under the acromion) are also defined as risk factors.
Diagnosis of a rotator cuff injury
Magnetic resonance imaging is the safest method for detecting a tear, but also partial tears of the rotator cuff. Ultrasound diagnostics is also important, as it enables a dynamic examination (visualization in motion). X-rays provide a good bony overview of the shoulder and can show osteoarthritis in the AC joint (acromioclavicular joint), the shoulder joint and also calcific foci very well.
Treatment of a rotator cuff injury
In younger patients, rotator cuff injuries should be treated surgically. Partial tears, but especially complete tears (transmural ruptures), usually do not close over time, as the pull of the affected muscle leads to further separation (dehiscence) of the tendon. Over the course of 5 years, the tears usually become larger and should therefore be surgically sutured (refixed), especially in younger people. In older people and if the injury has been present for some time, the muscle belly can become fatty (arthrophy) due to a lack of activity. Despite a successful rotator cuff suture (refixation), the desired result may not be achieved and a loss of strength may persist. Even if a complete reconstruction no longer appears possible, a partial tendon suture can usually achieve a significant improvement in mobility and discomfort.
In older patients with a non-dominant hand and no overhead work, a three-month conservative treatment trial with physiotherapy can be attempted. The intact tendons can compensate for the sometimes minimal loss of function. In this way, good mobility and freedom from pain can be achieved. If pain persists and movement is restricted, surgery should not be delayed for too long.
Procedure for rotator cuff surgery
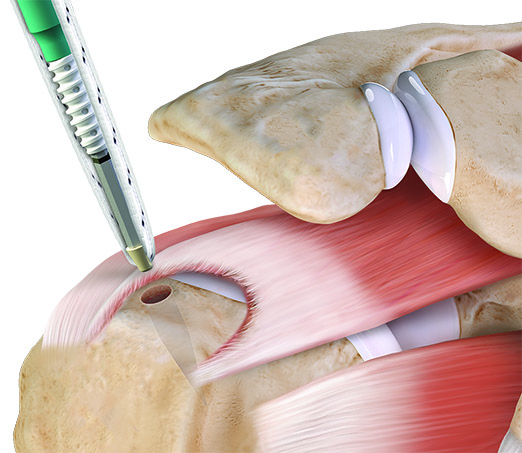
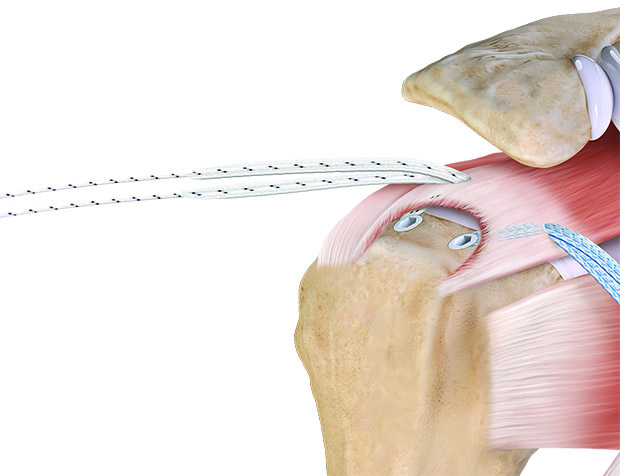
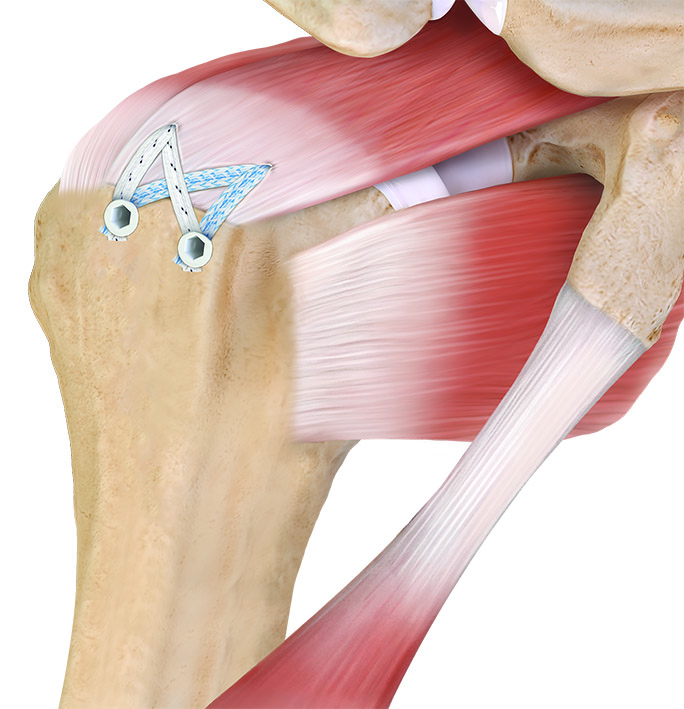
I perform this operation arthroscopically (keyhole technique) in almost all cases, so that only a few 1 cm scars remain. A so-called mini open procedure (additional 5 cm incision) is only required in exceptional cases. The patient is placed in a semi-sitting position on the operating table (beach chair position) and a standardized arthroscopy of the shoulder joint is performed. The entire joint is examined in order to view all parts of the rotator cuff. Here I place particular emphasis on the assessment of the subscapularis tendon (= anterior part of the rotator cuff), as tears in this tendon are very frequently overlooked.
The bursa subacromialis is then removed below the acromion and a downward protruding bone spur (subacromial impingement) is removed. Several suture anchors are now inserted into the humerus and the sutures are passed through the torn tendon. This allows the tendon to be reattached to its original attachment to the humerus
Aftercare
A so-called abduction cushion bandage is applied in the operating theater, which must be worn consistently for 6 weeks in most cases. In the initial phase, only passive movements may be performed, which must be worked out with the physiotherapist. Of course, the follow-up treatment can be individually adapted depending on the size of the tear and the quality of the tendon.

{kind=link}
{kind=link}
{kind=link}